
QT Imaging’s opportunity in breast imaging is to speed the time to diagnosis for women with cancer, and to provide assurance for women who do not have the disease with a better patient experience and lower cost than the current standard of care.
QTI Breast Acoustic CTTM System has no reports of adverse effects from the 15,000 scans performed to date. Similar to other ultrasound devices including handheld devices, there are no known significant risks reported in general clinical practice. The QT Breast Acoustic CTTM Scanner does not require potentially harmful ionizing radiation or anesthesia and is done in an open environment thereby decreasing stress and the necessity of sedation. As a result, there is the potential for increased imaging efficacy. Additionally, the scanner does not cause breast implant displacement or rupture.
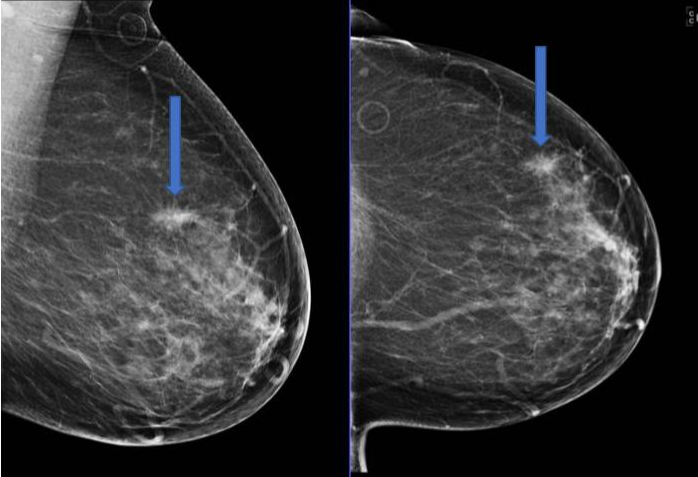
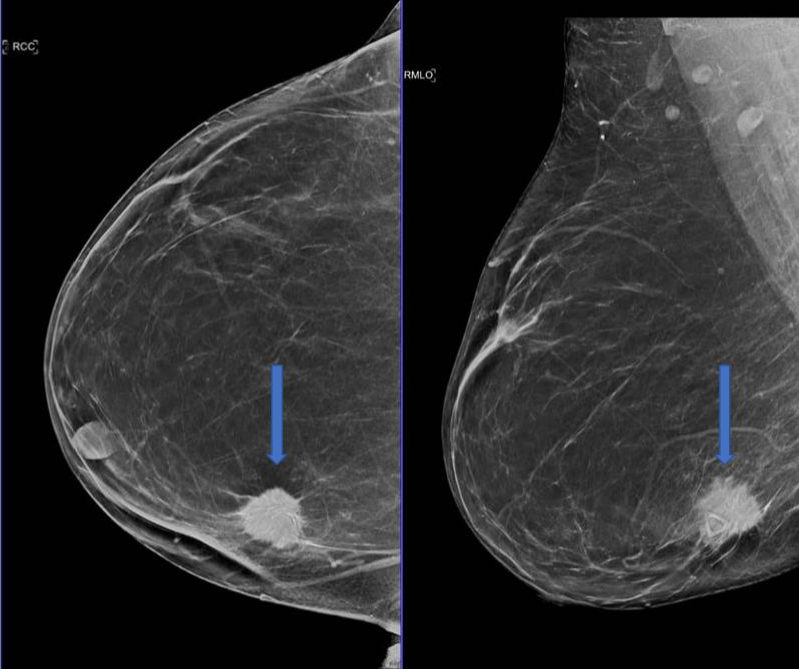
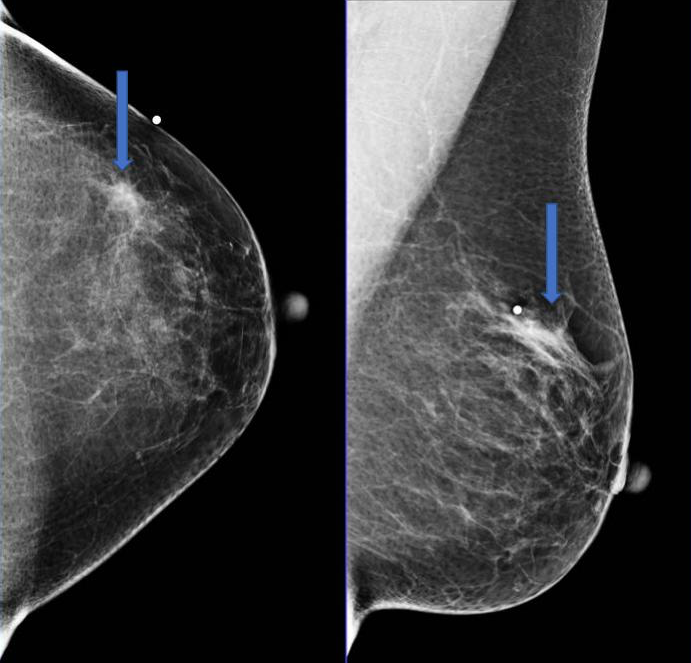
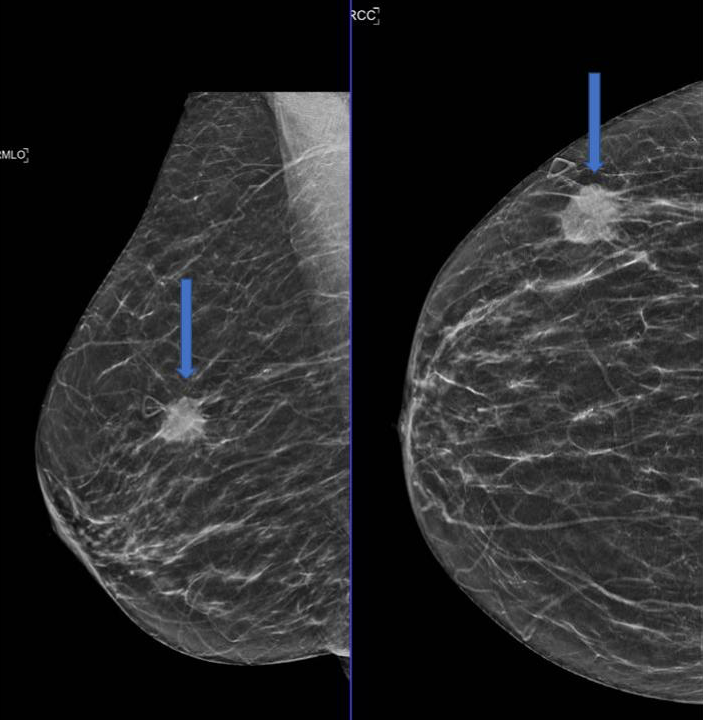
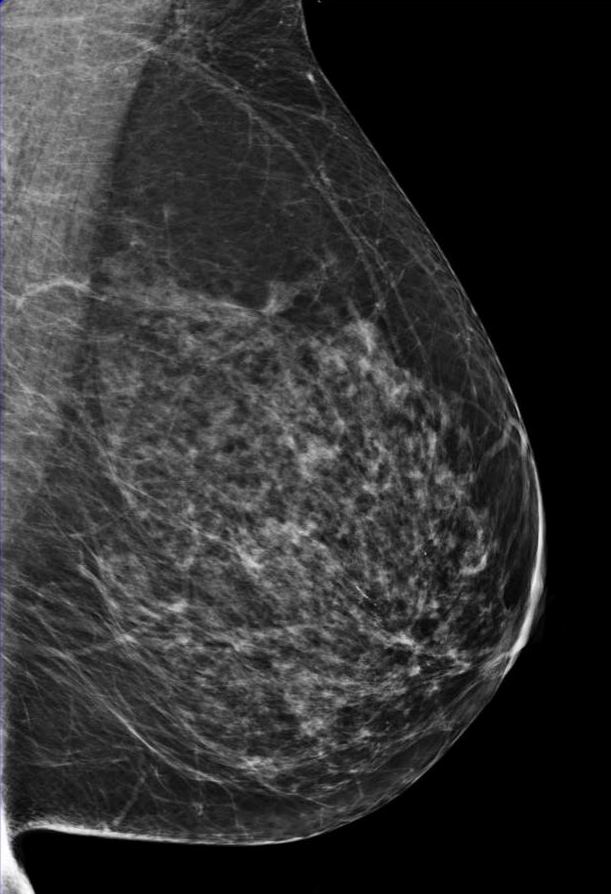
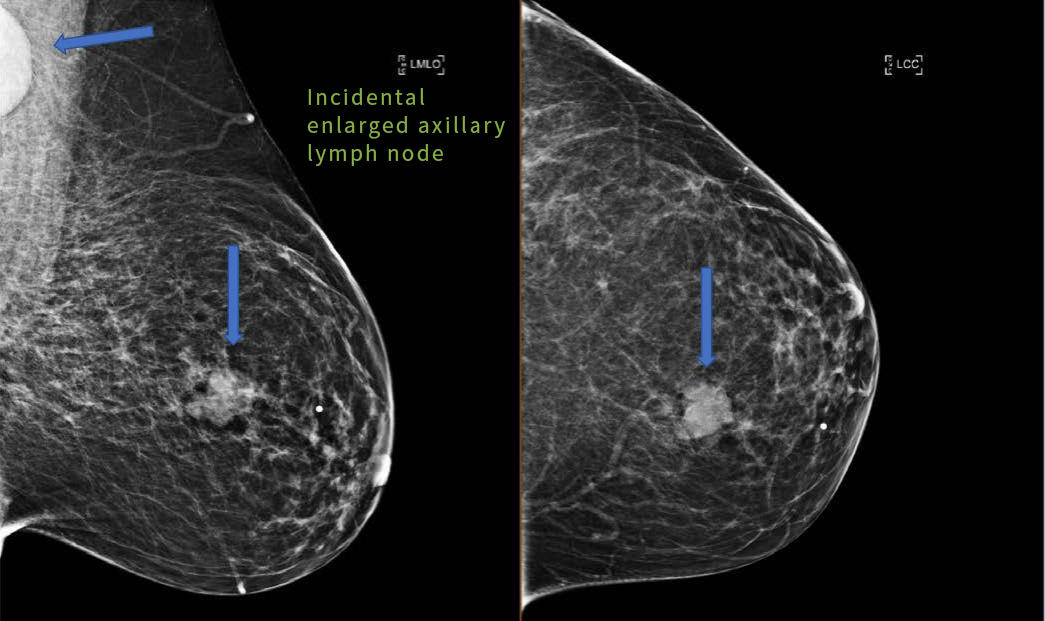
Spiculated focal asymmetry.

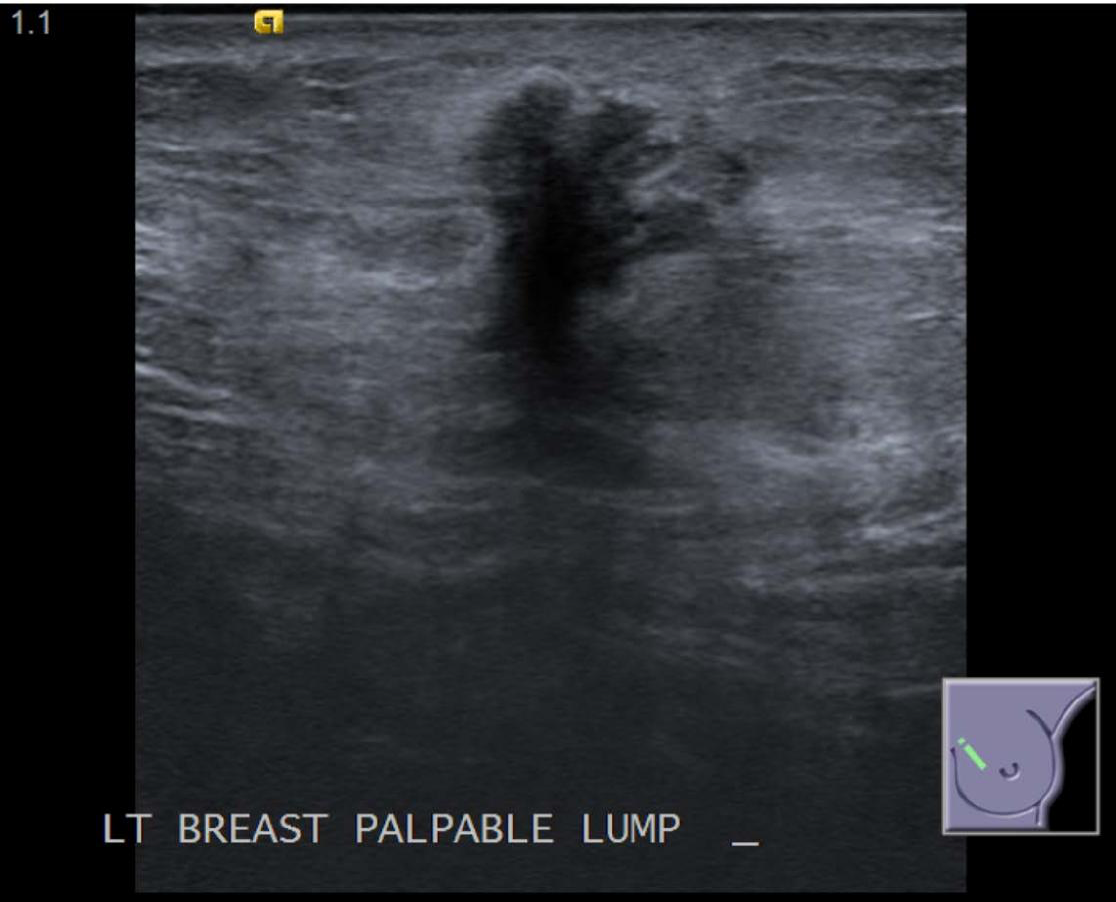
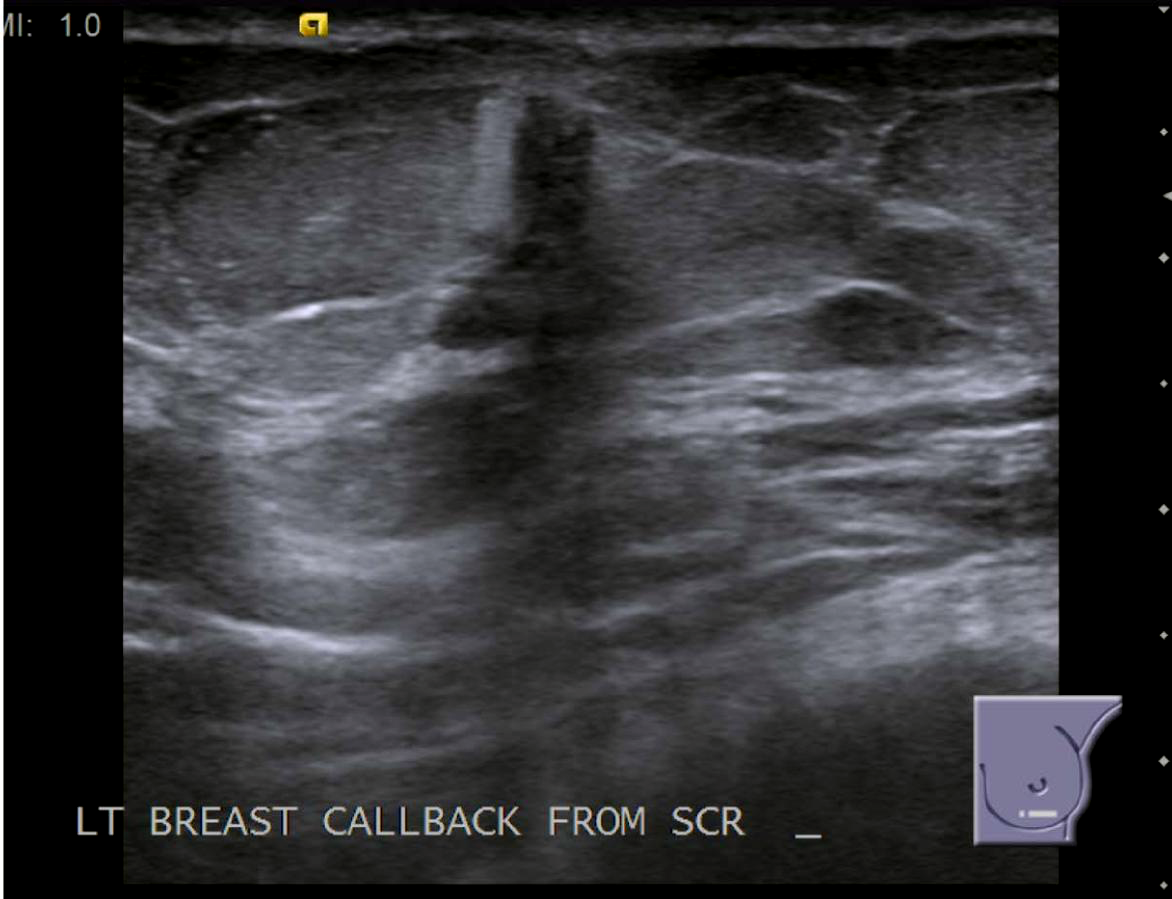
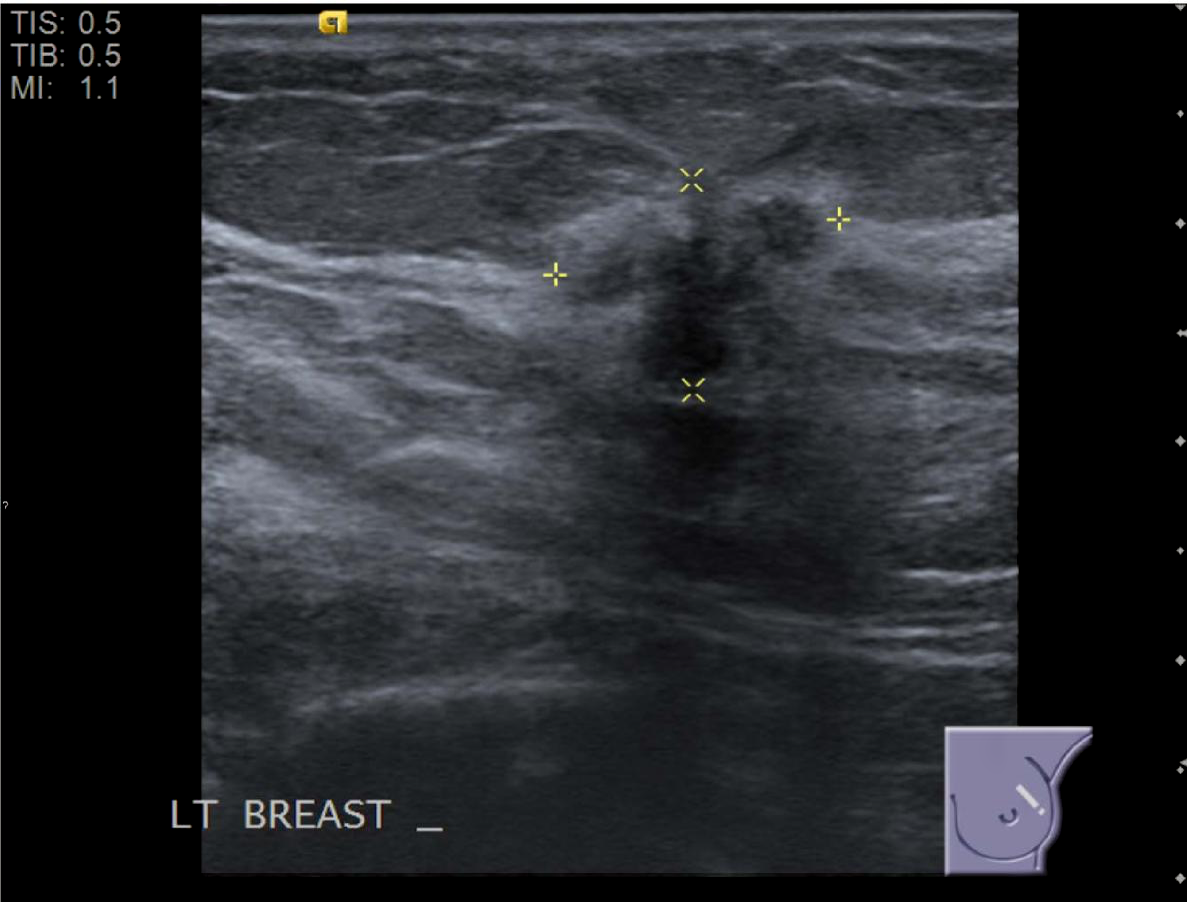
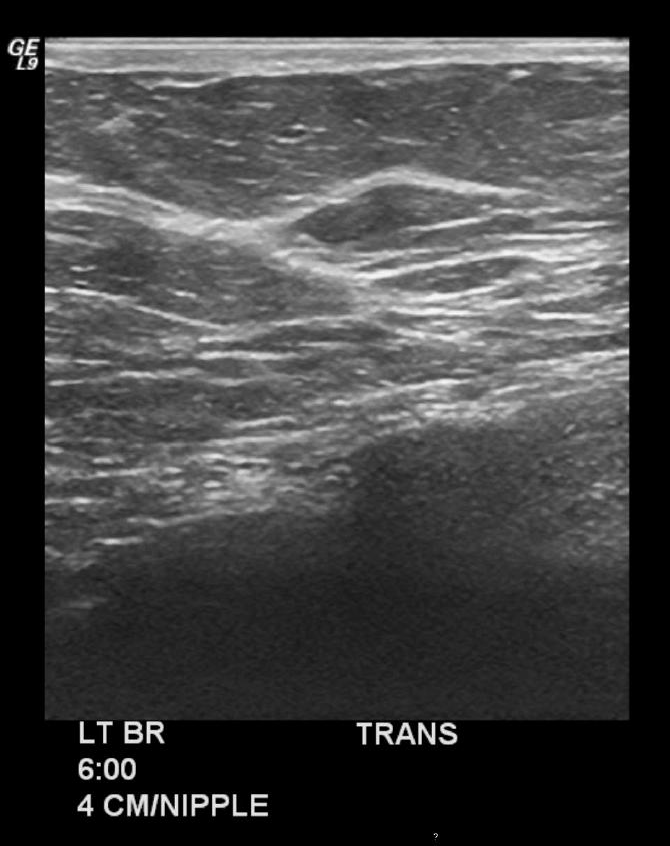
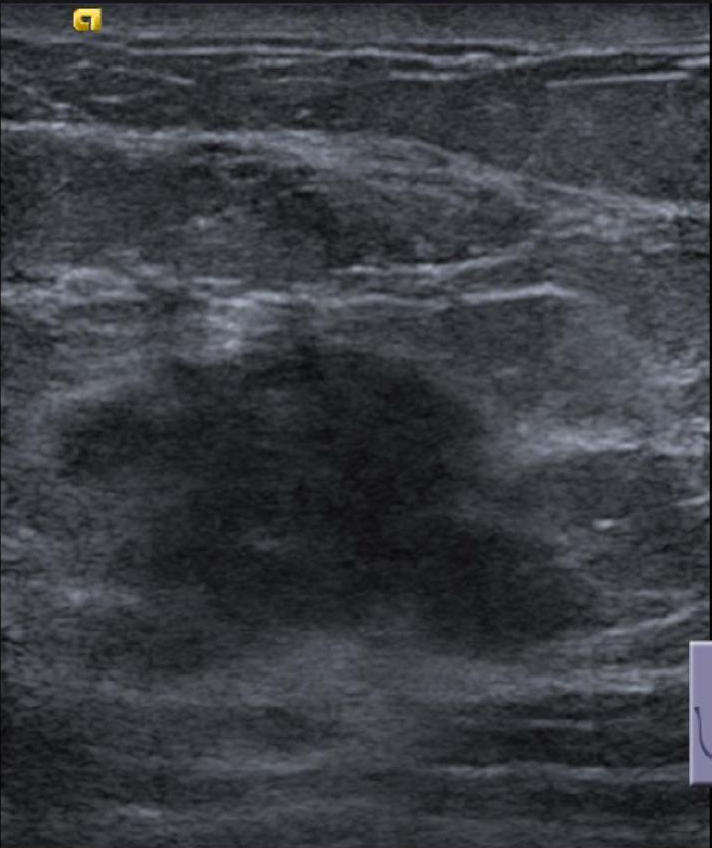
Irregular, hypoechoic solid mass. Echogenic halo.
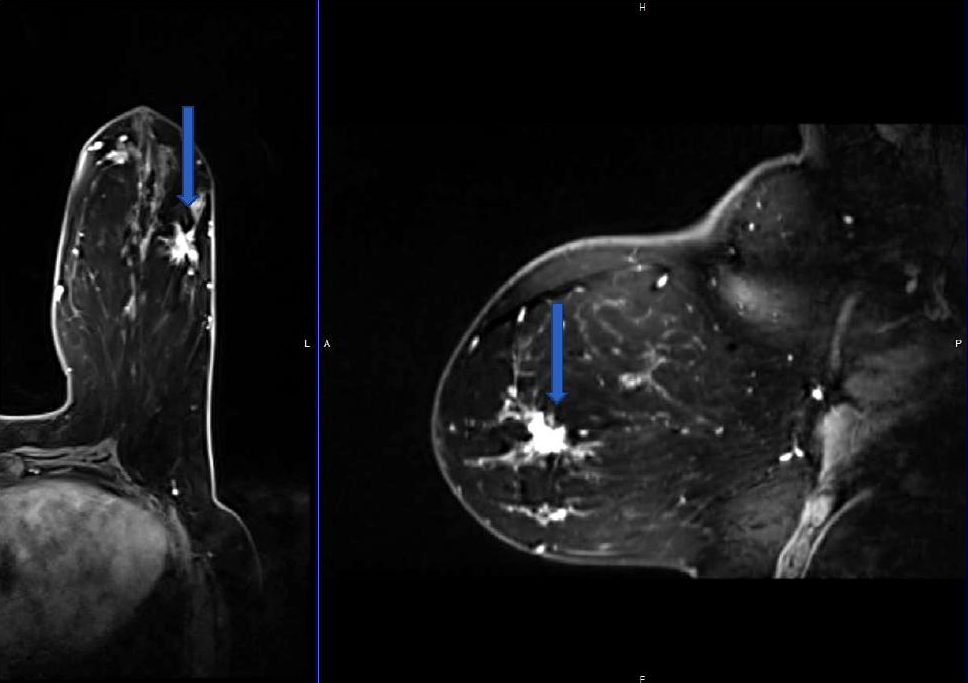
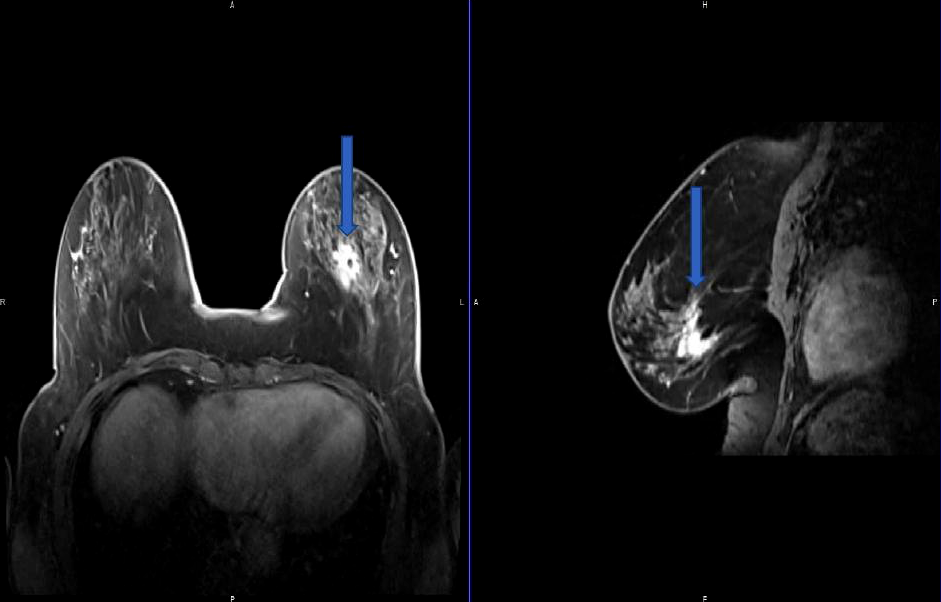
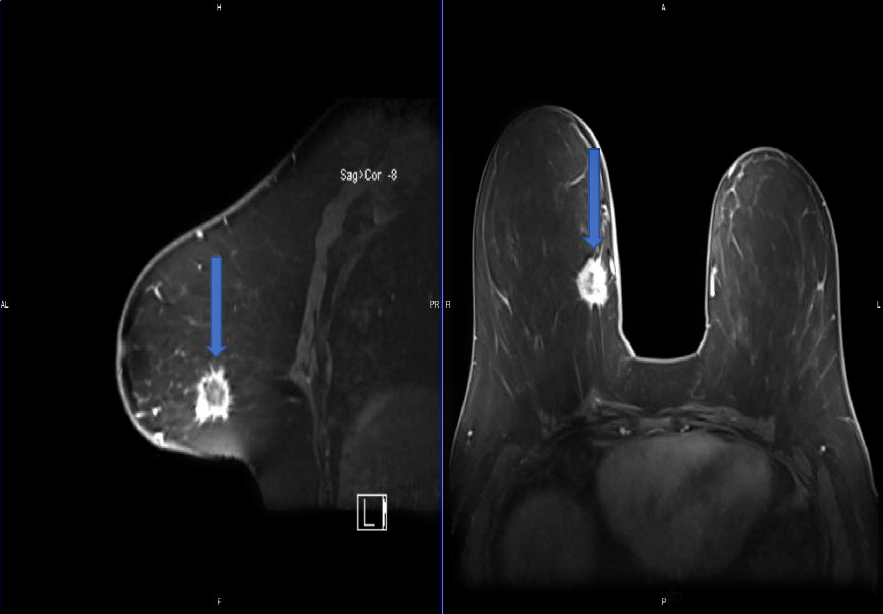
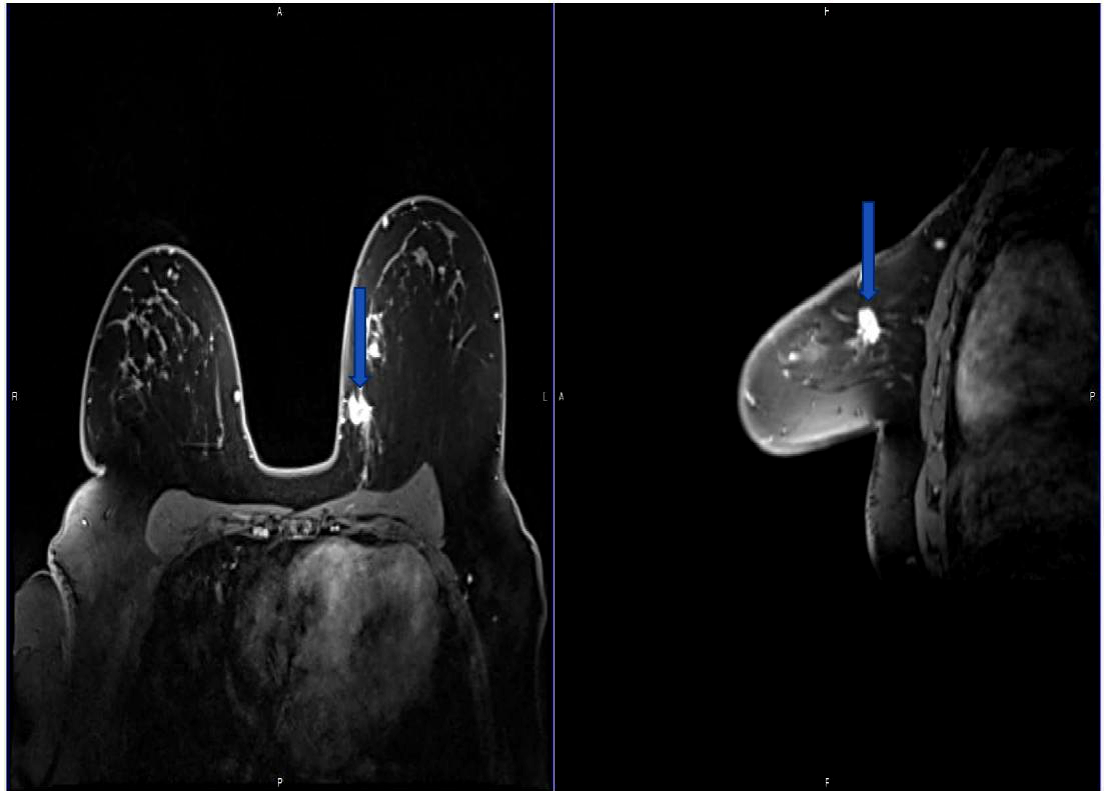
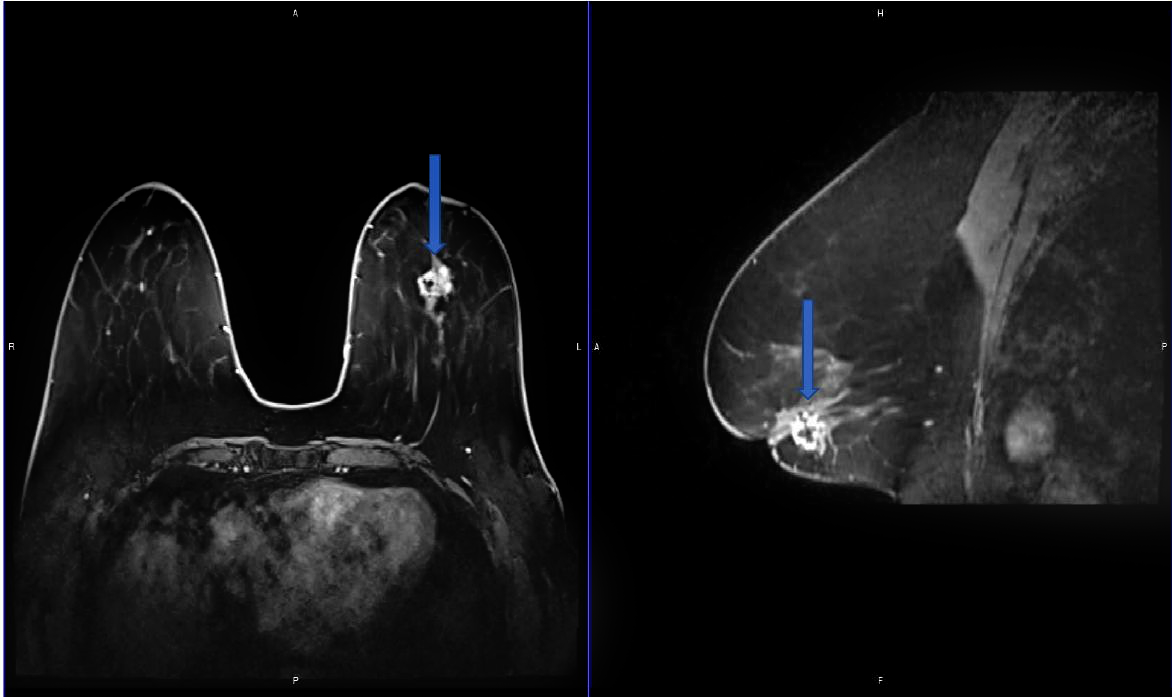
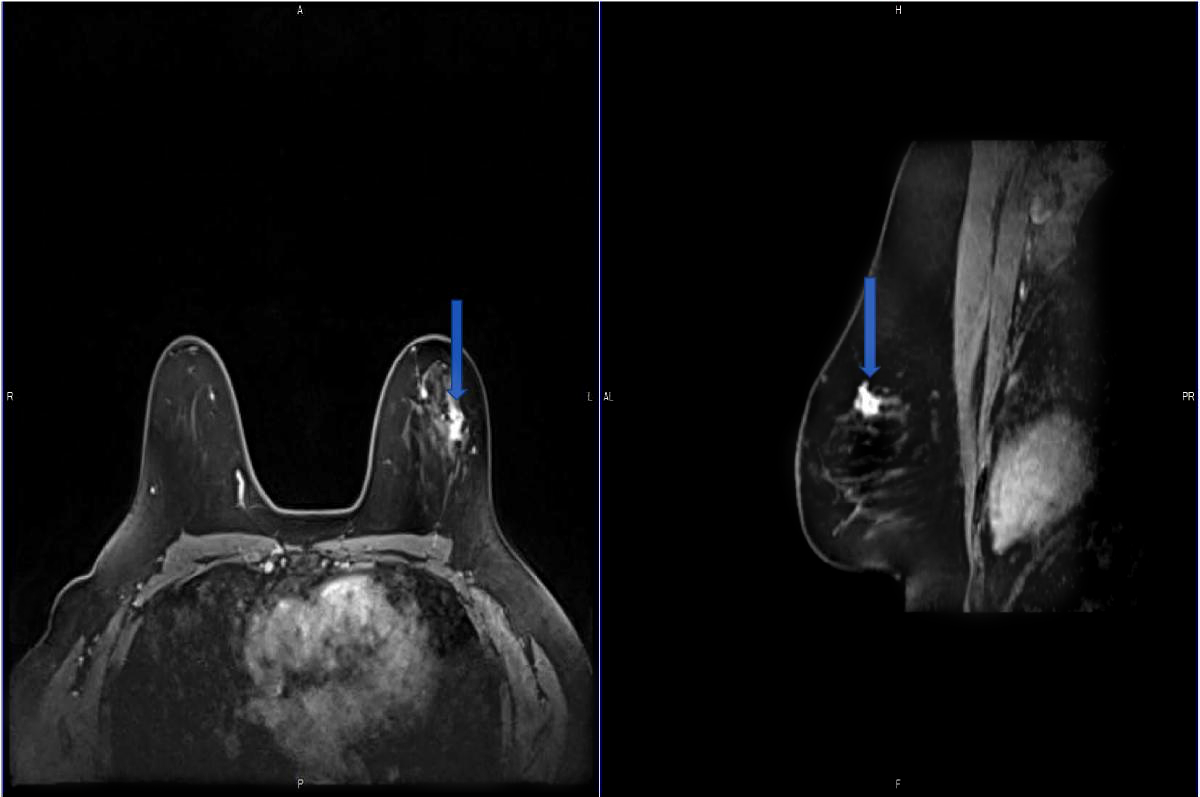
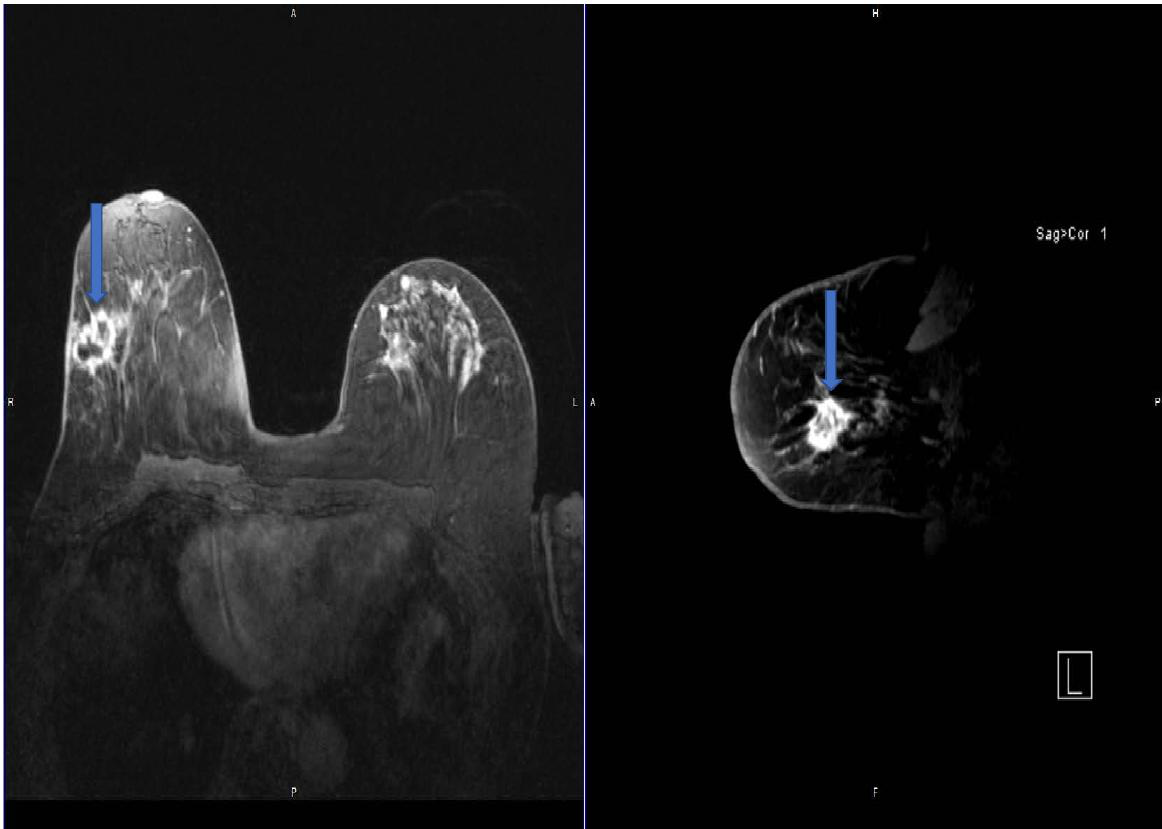
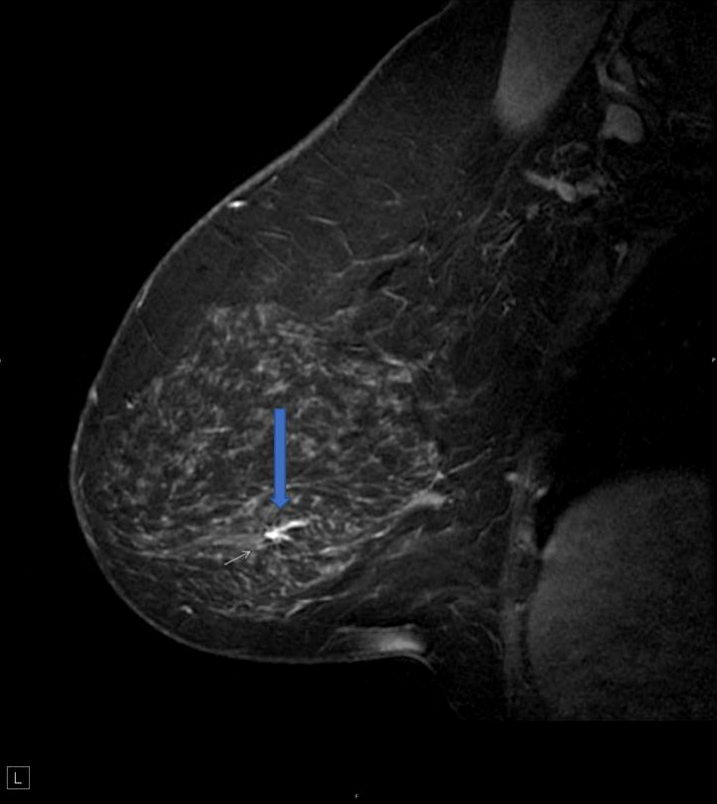
Irregular, spiculated mass demonstrating suspicious enhancement kinetics.
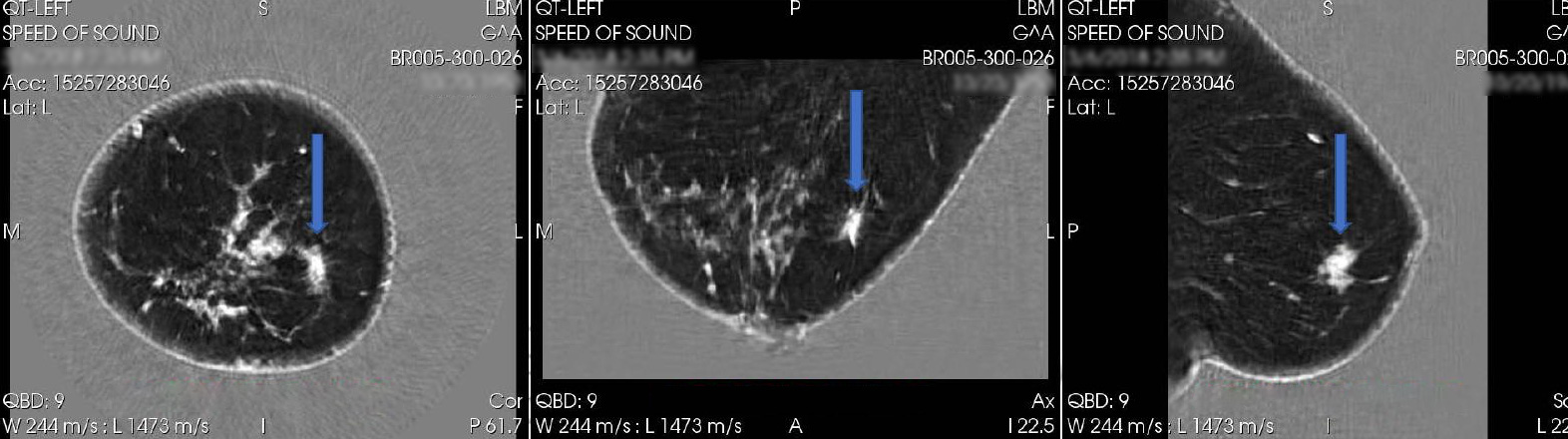
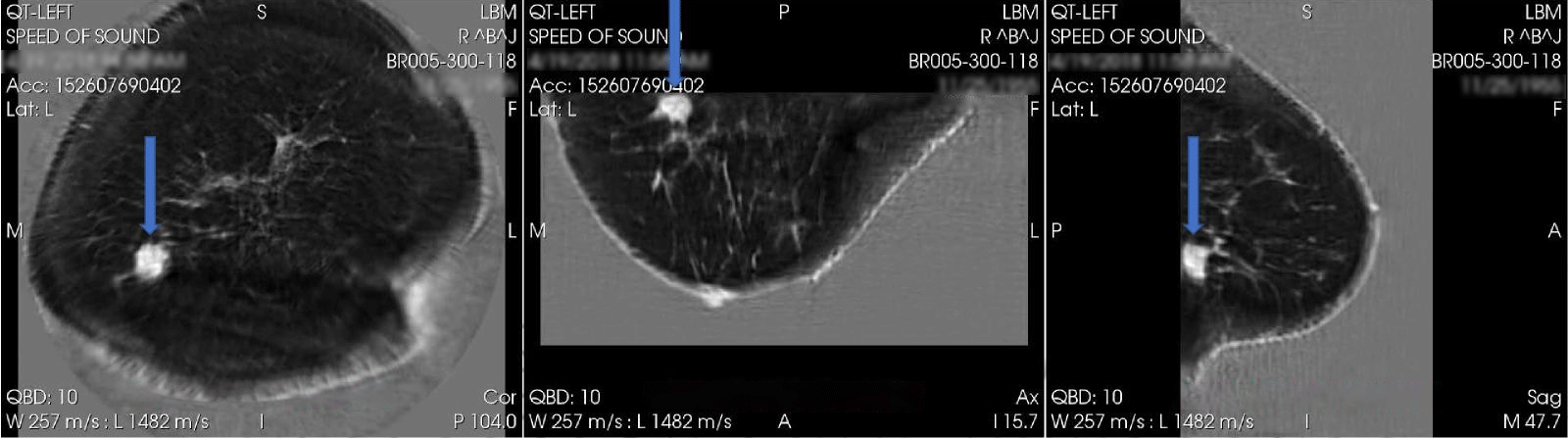
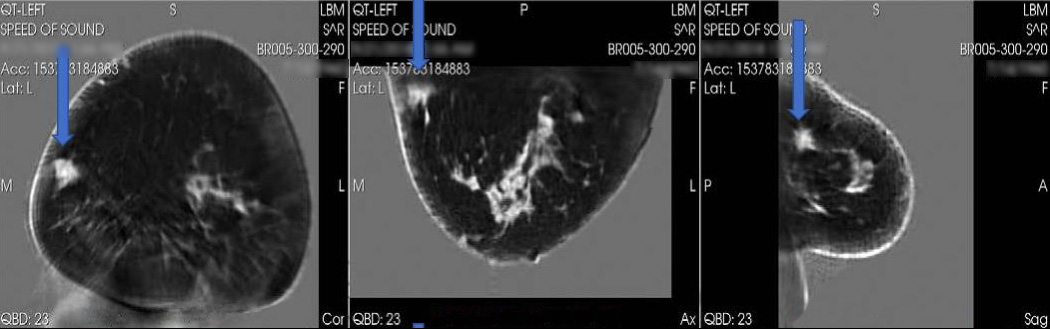
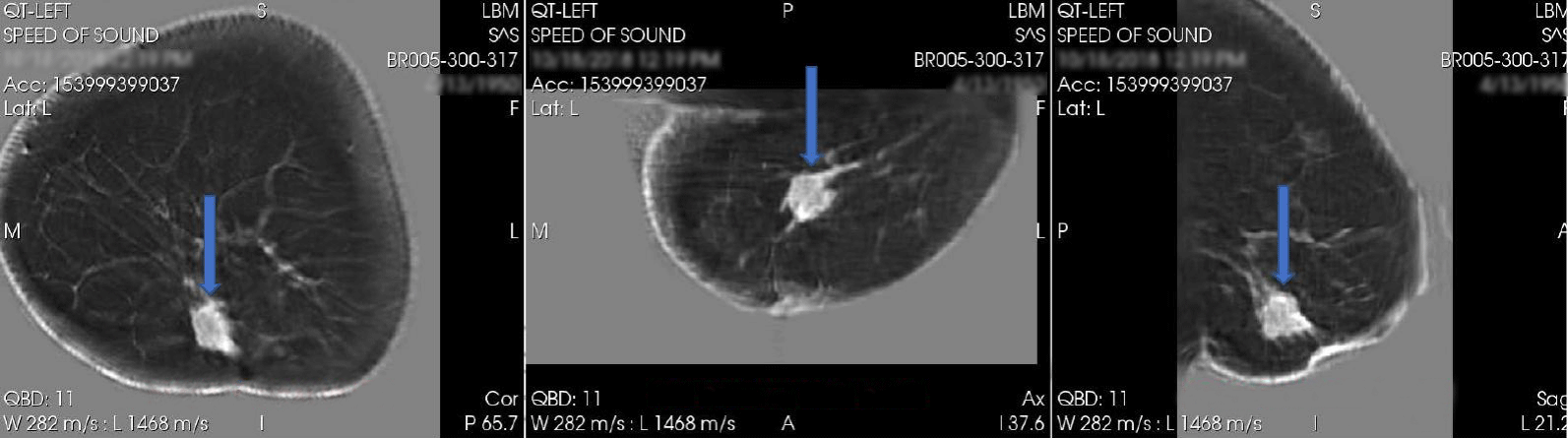
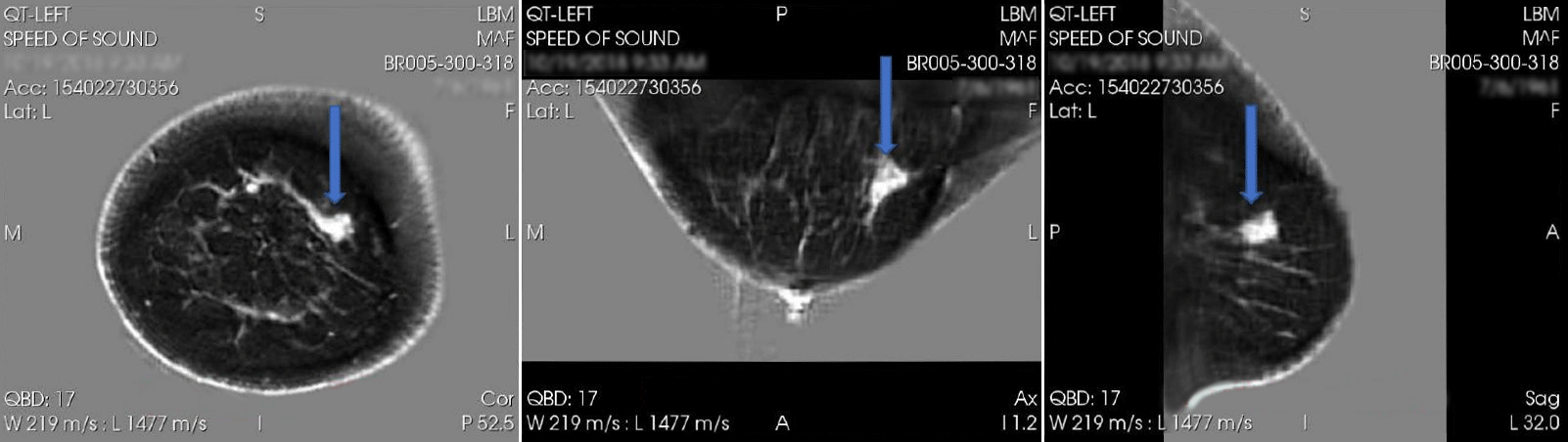
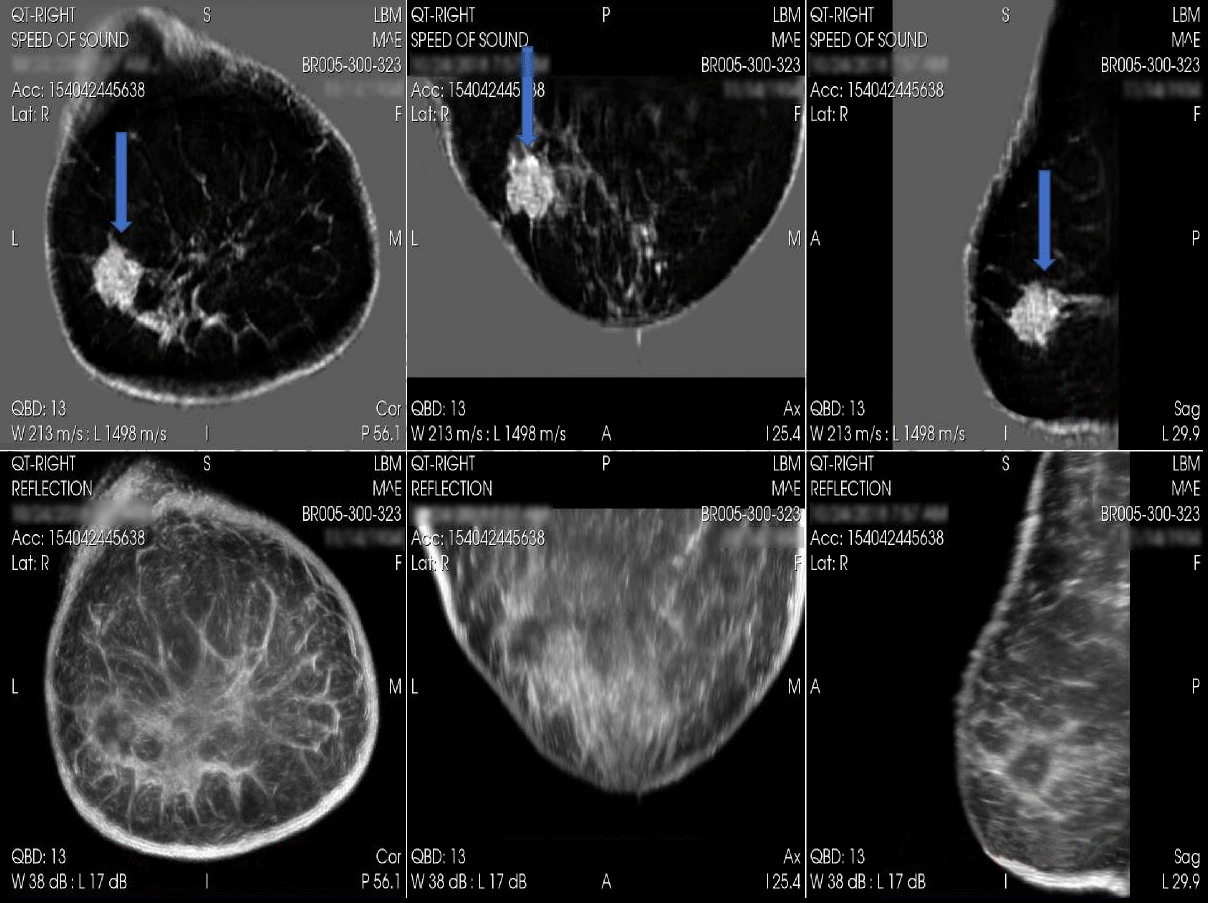
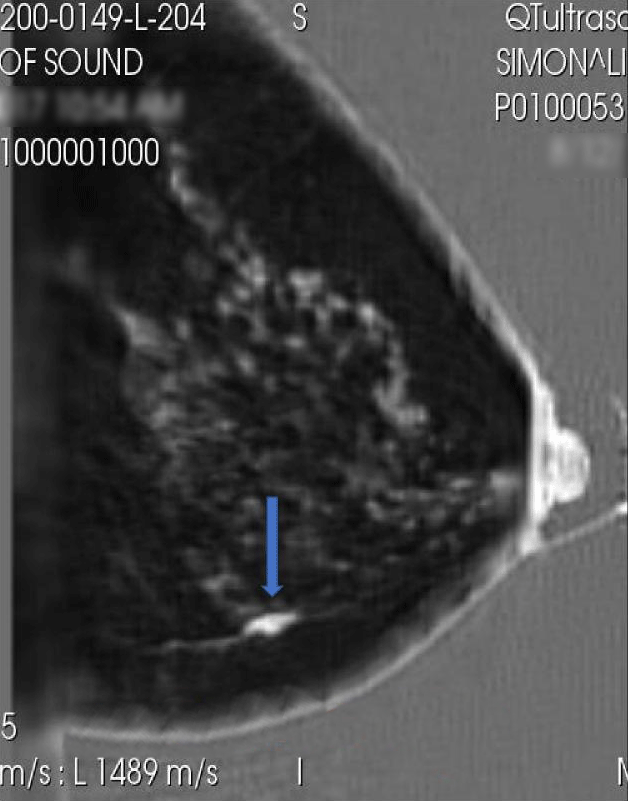
Irregular, high speed mass.
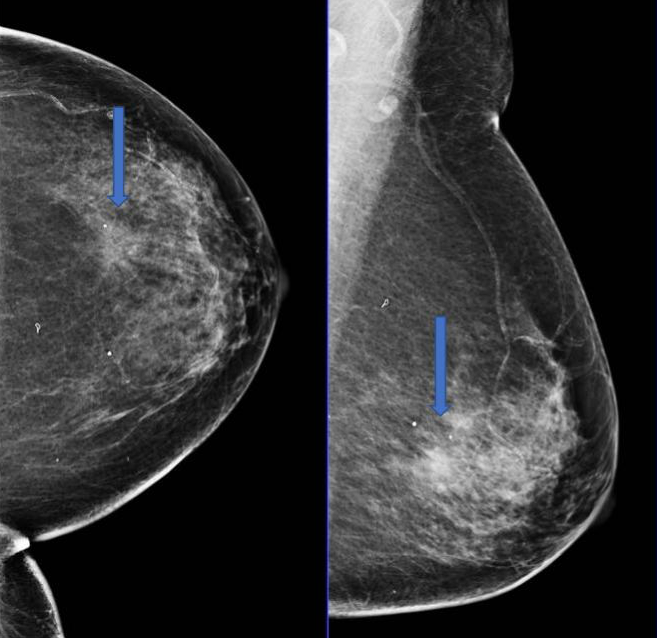
Focal asymmetry, subtle finding mammographic ally due to adjacent dense breast tissue.
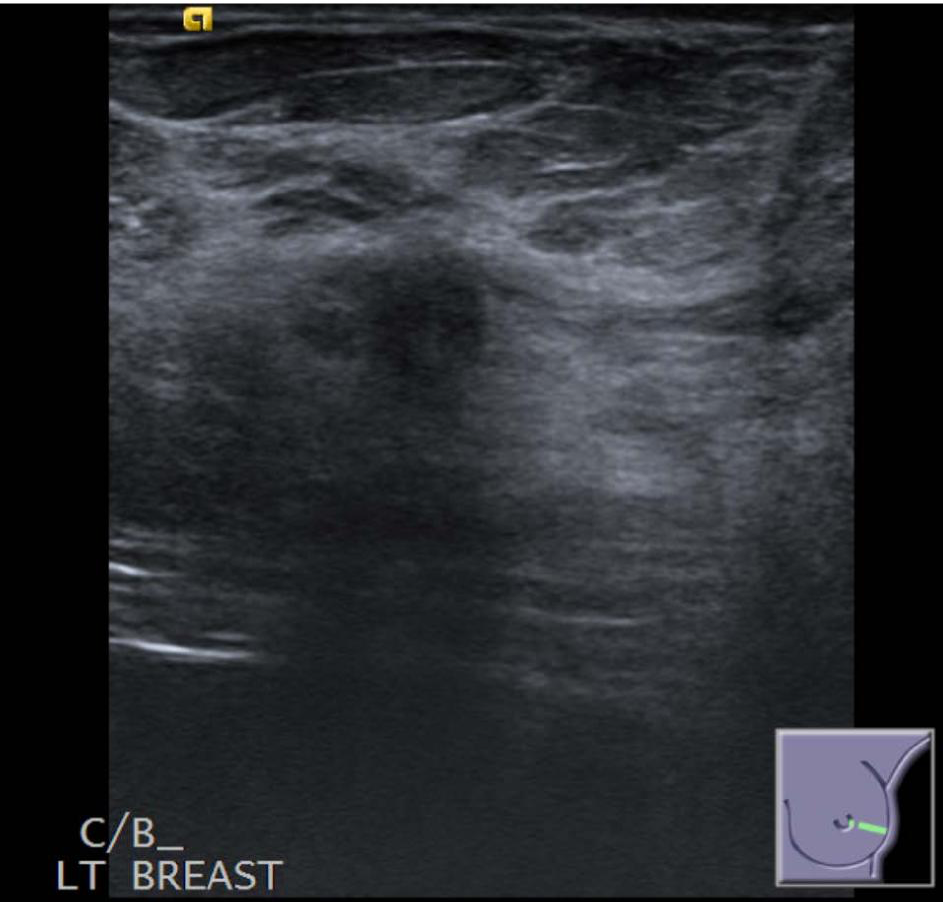
Ill-defined, subtle hypoechoic mass detected sonographically.
Posterior acoustic shadowing.
Irregular, solid mass.
Suspicious enhancement kinetics.

High speed mass is confirmed on QTScan™, extent of disease more precisely mimics that of MRI, larger than area appreciated on mammography or handheld ultrasound.
Irregular, spiculated mass.
Easy to see mammographically due to fatty breast tissue.
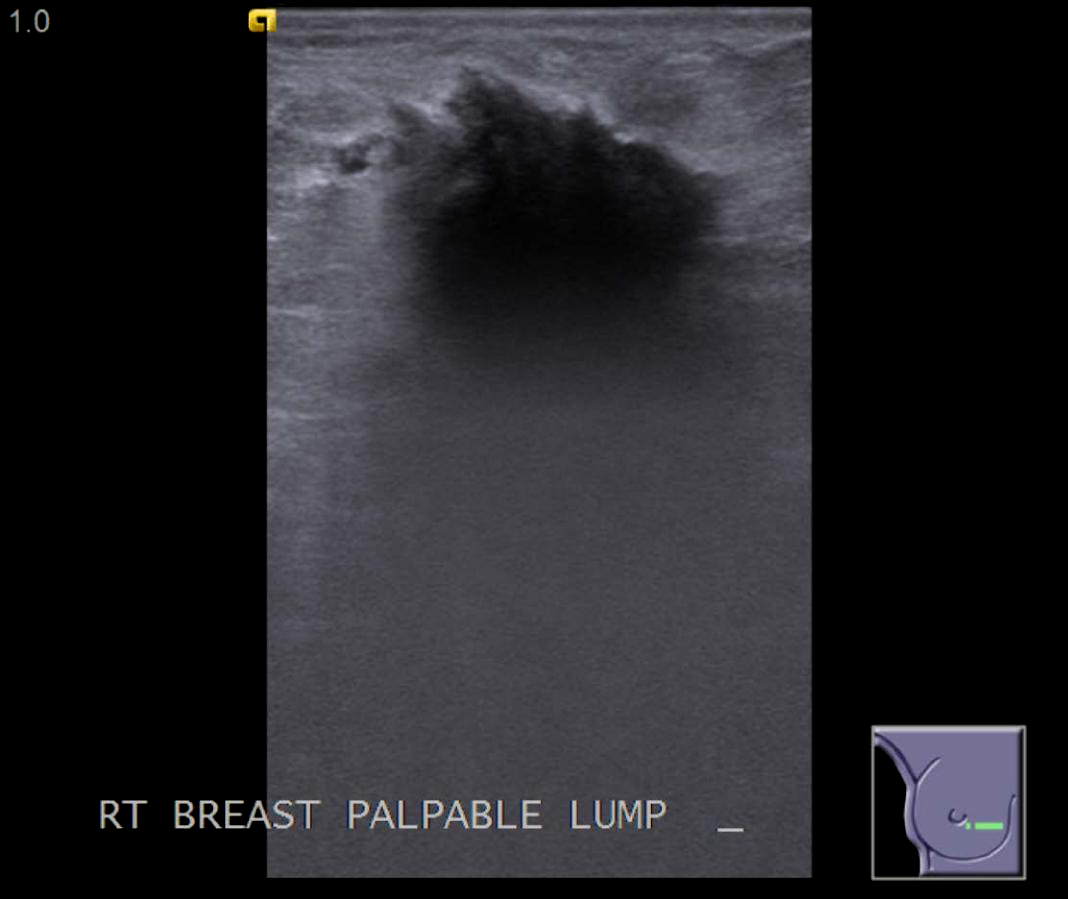
Irregular, hypoechoic solid mass.
Posterior aspect of the mass not clearly visualized due to posterior acoustic shadowing.
Irregular, spiculated mass confirmed on with peripheral enhancement.
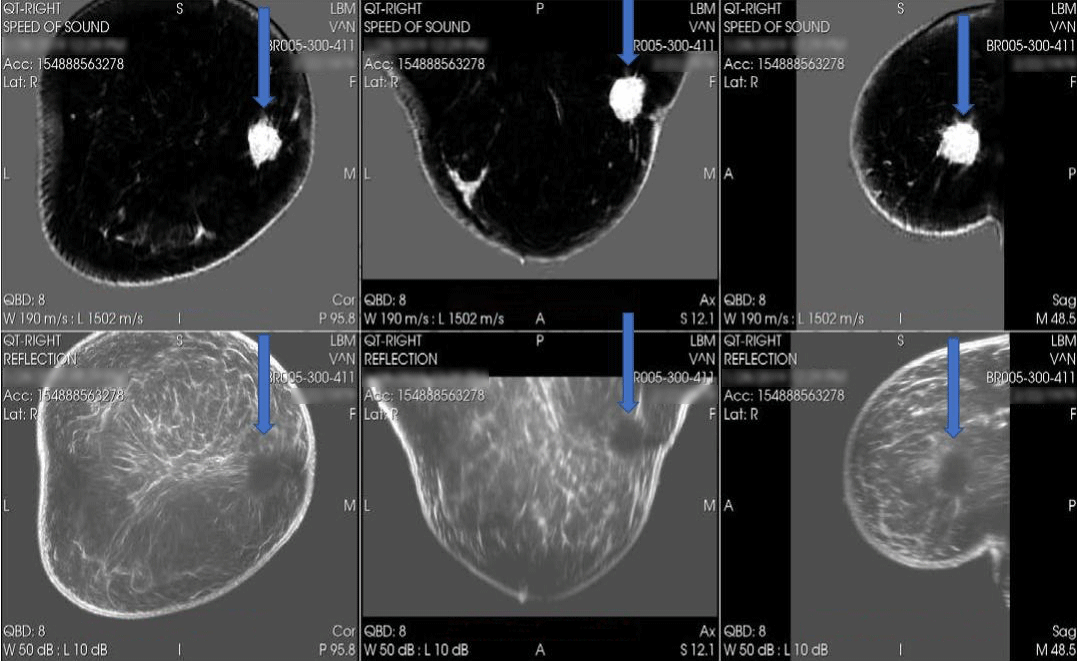
Spiculation/distortion on reflection. Mass visualized in its entirety, as opposed to handheld ultrasound technology.
High speed. Spiculations on transmission images; distortion well seen on reflection.
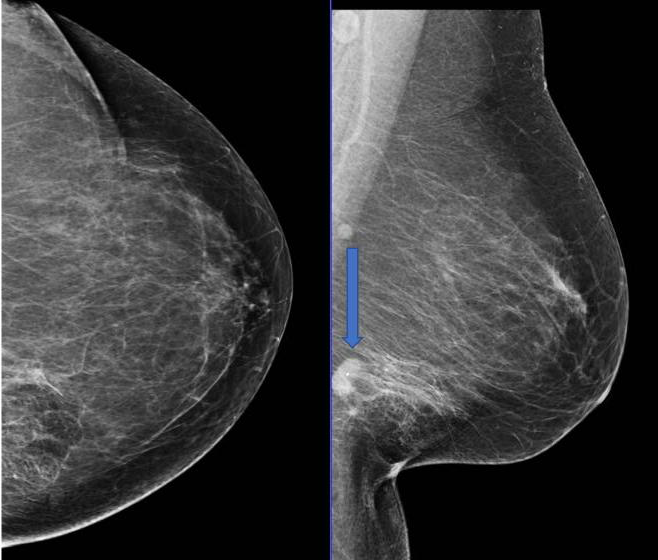
Mass cut off on CC view due to its posterior location and therefore not visualized.
Mass seen in the posteroinferior left breast on MLO view.
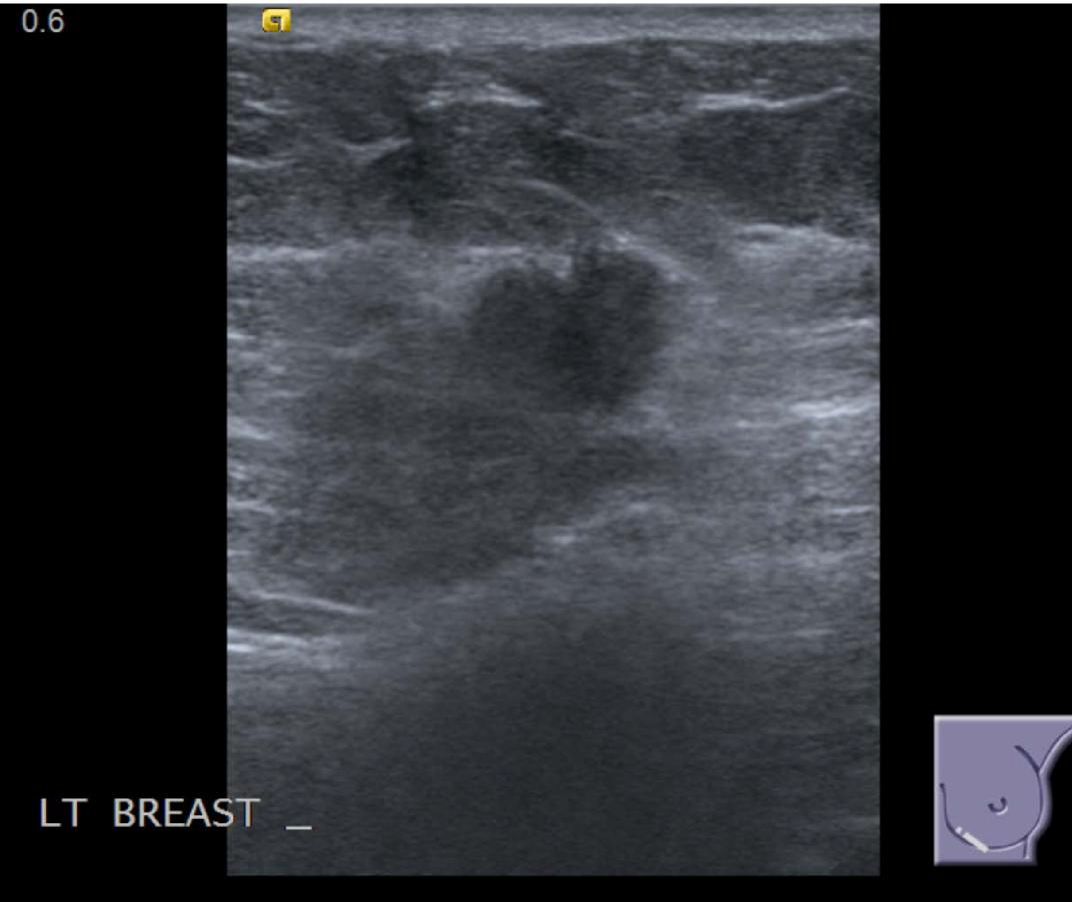
Solid, hypoechoic mass confirmed sonographically.
Margins poorly visualized on handheld.

Irregular, suspiciously enhancing mass confirmed on MRI.
Entire mass visualized in the lower inner quadrant posteriorly. Margins of mass clearly visualized. Areas of spiculation noted.

Irregular mass at 9:00.
Subtle finding on MG.
Solid, hypoechoic, irregular mass confirmed on ultrasound.
Posterior aspect of mass not well visualized due to posterior acoustic shadowing.
Suspiciously enhancing, irregular mass confirmed on MRI.
Irregular, high speed mass seen on speed images.
Corresponding hypoechoic mass is identified on reflection images.
Distortion well seen on reflection.

Ill-defined, low density focal asymmetry.
Given the low density, may not look very suspicious mammographically.
Solid, hypoechoic mass is confirmed sonographically.
Taller than wide.
Echogenic halo.
Posterior acoustic shadowing.
Irregular, heterogeneously enhancing mass is confirmed.
Low speed mass with high speed irregular periphery.
Spiculation seen on sagittal.
Borders not well visualized.
Irregular margins.
Not cyst.
Focal asymmetry in the area of lump in the upper outer quadrant of the left breast.
Hypoechoic, irregular solid mass is confirmed on handheld ultrasound.
Focal area demonstrating suspicious enhancement kinetics is identified on MRI.
Focal high speed space-occupying lesion.
Closely mimics the extent of disease identified on MRI.
Spiculated mass.
Well seen in background of scattered fibroglandular tissue on mammogram.

Large, solid necrotic mass is identified sonographically.
Heterogeneous mass with central necrosis confirmed on MRI.
Irregular, low speed mass is identified.
Low speed may be due to central necrosis/fluid inside.
Corresponding hypoechoic mass on reflection, margins well seen.
Thick echogenic halo on reflection.
ILC not seen on Mammogram.
ILC not seen on handheld.
ILC seen on MRI.
Focal linear, branching homogeneous non mass-like enhancement.
ILCA seen on QT.
Fusiform space-occupying lesion noted on QT, looks similar to MRI.
Lobulated mass is identified.
Adjacent satellite nodules are not appreciated mammographic ally.
Lobulated, hypoechoic solid mass is confirmed on handheld ultrasound.
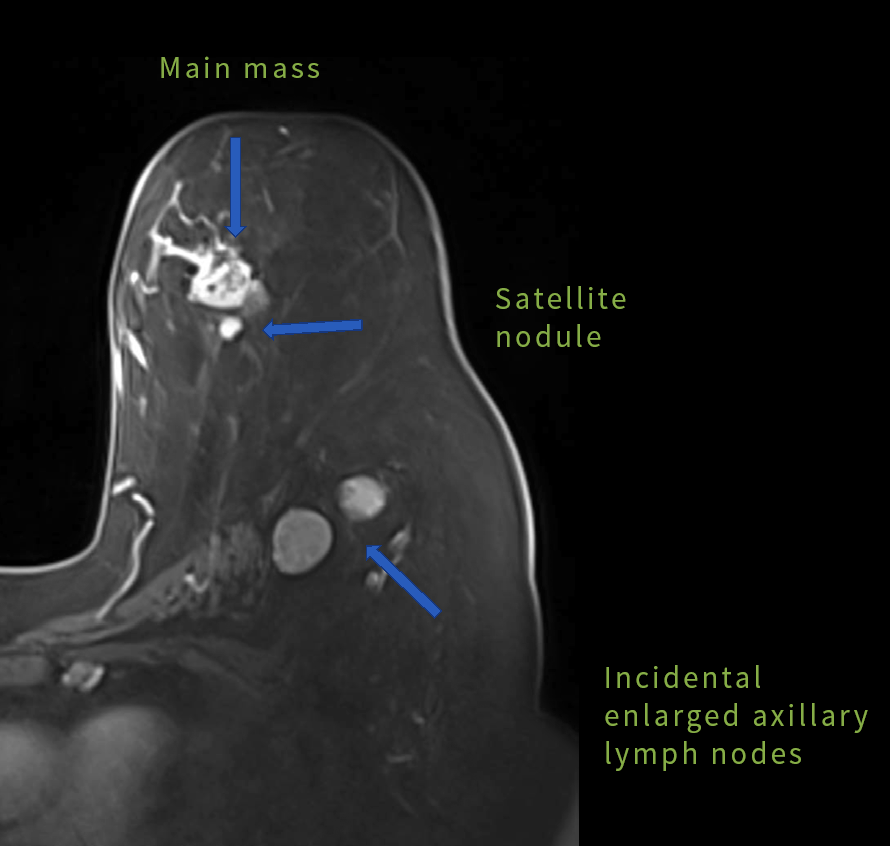
IDC seen on MRI.
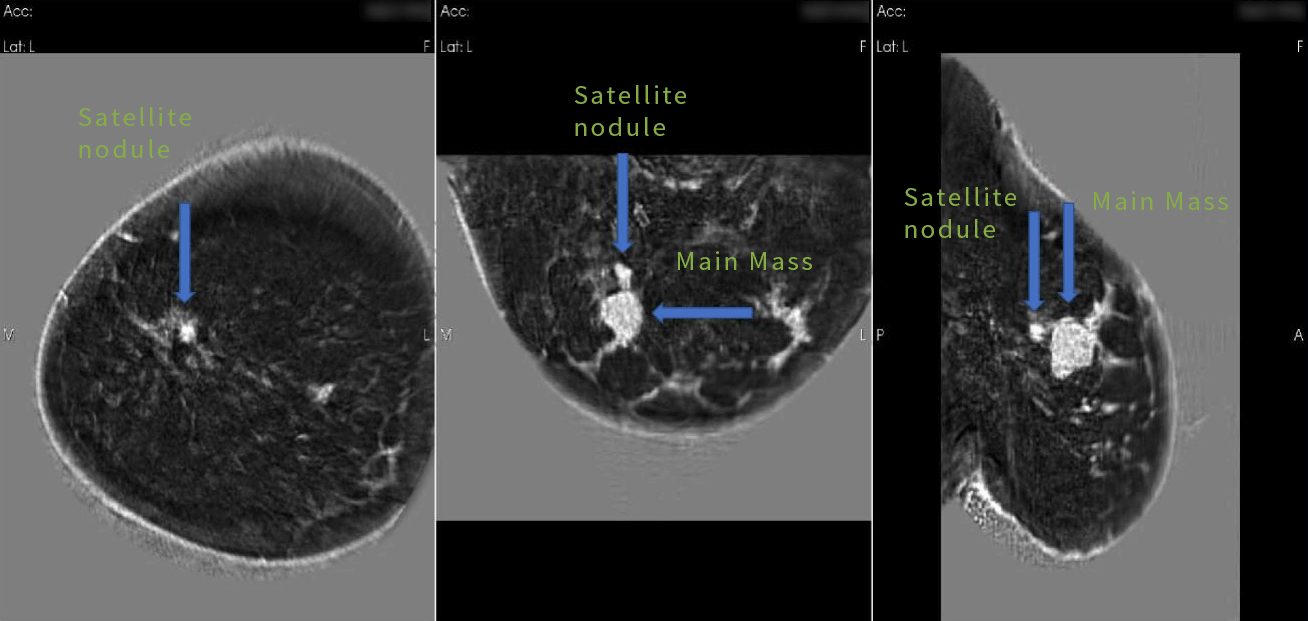
IDC seen on QT.
Main mass with adjacent satellite modules.
Similar to MRI.